| Video Discription |
Here is a case of a 49 year old man with a history of alcohol related liver disease who presented with acute upper GI bleeding and required urgent out of hours endoscopy in the A&E department. A potted history is as follows:
7 yrs ago: squamous cell carcinoma of tongue diagnosed, Rx wide local resection, no radiotherapy, currently in remission.
3 yrs ago: cerebellar ataxia and cerebral atrophy, conservative management.
7 months ago:
- Admitted with decompensated alcoholic cirrhosis (drinking 30-50 u/week)
- Moderate ascites, oedema, no PSE, no SBP
- Bilirubin 65 umol/L, ALT 72, Alt Phosp 620 (NR less than 130)
- Alb 25, INR 0.9, Hb 127 g/L, WBC 15, Platelets 86
- MELD-Na: 11, Child-Pugh class C (11/15)
- U/S: diffuse liver disease, normal PV flow, no splenomegaly
- Cardiac echo: ejection fraction 65%
- Rx Spironolactone / Frusemide
- Continued drinking alcohol 50u/week after discharge
- Out patient OGD planned but not done
Now:
- Admitted with 3 days of melaena + 2 days bright haematemesis
- Worsening jaundice for 2 weeks
- Taking Anadin for abdominal pain
- 1 litre haematemesis in A&E
- HR 120 - 130 BPM, BP 130/80 mm Hg
- Hb 86 g/L (was 120), WBC 20.2, platelets 114, INR 1.5, Alb 26
- Urea 9.1 (was 3.5)
- Bilirubin 212 umol/L, ALT 37, Alt Phosp 303
- MELD-Na: 21, Child-Pugh class C (11/15)
- Major haemorrhage protocol activated ... Rx 3 units blood
- Rx Terlipressin, iv PPI
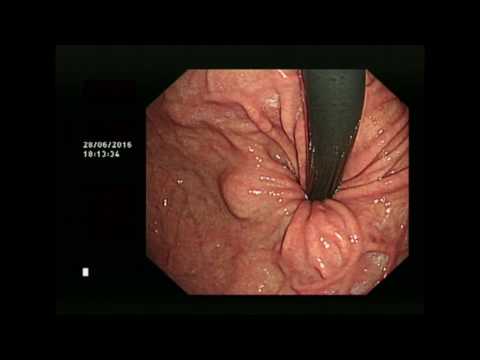
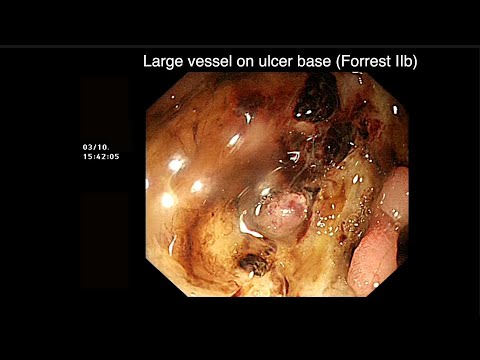
Urgent out of hours OGD in A&E (after Erythromycin 500mg iv)… see video
—
The prevalence of gastric varices (GV) is estimated between 17% and 25% in patients with portal hypertension (pHTN) in comparison with oesophageal varices (OV), which are present in up to 85% of these patients. Although OV are more prevalent and bleed more frequently, haemorrhage from GV bleeding is often more severe, with an incidence of 16%–45% at 3 years, and associated with higher mortality.Similar rates of bleeding and mortality from GV are reported for patients with non-cirrhotic compared with cirrhotic pHTN.
In practice, most gastroenterologists classify GV using the the Sarin system:
- GOV1 (OV and lesser curve GV),
- GOV2 (OV and cardiofundal GV),
- IGV1 (cardiofundal GV without OV) and
- IGV2 (distal GV without OV).
GV can also be classified by risk of bleeding. While Sarin has identified cardiofundal GV as being higher risk for bleeding, other groups have identified GV size, presence of a red mark, or discolouration as risk factors of bleeding, analogous to the North Italian Endoscopic Club criteria for predicting EV bleeding.
Regarding management of variceal bleeding, the main recommendations of the recently published ESGE guidelines are listed below [1]. Recommendations 12-14 are of particular interest in cases of bleeding from GV. Note that EBL or cyanoacrylate glue is recommended for GOV1 specific bleed.
continued in first comment... |