Laparoscopic totally extra-peritoneal (TEP) inguinal hernia repair #drshivkumarbunkar #surgery
Hellow guys, Welcome to my website, and you are watching Laparoscopic totally extra-peritoneal (TEP) inguinal hernia repair #drshivkumarbunkar #surgery. and this vIdeo is uploaded by Dr Shiv Kumar Bunkar at 2023-01-16T22:36:52-08:00. We are pramote this video only for entertainment and educational perpose only. So, I hop you like our website.
Info About This Video
| Name |
Laparoscopic totally extra-peritoneal (TEP) inguinal hernia repair #drshivkumarbunkar #surgery |
| Video Uploader |
Video From Dr Shiv Kumar Bunkar |
| Upload Date |
This Video Uploaded At 17-01-2023 06:36:52 |
| Video Discription |
Laparoscopic totally extraperitoneal (TEP) inguinal hernia repair is an effective minimally invasive method for treating hernias that avoids entry into the abdomen. Its indications have developed and broadened over time to encompass almost the whole spectrum of groin hernias. A detailed description of the procedure is presented focusing on seven key steps. Moreover, pre- and intra-operative considerations, pearls and pitfalls are highlighted in order to maximize efficiency and safety when performing this procedure. The attached figures and accompanying narrated videos complement this manuscript by providing an audiovisual adjunct and to clarify technical and anatomical descriptions.
Steps of TEP
1. Identify the pubic symphysis in the midline
2. Bluntly dissect Cooper’s ligament bilaterally. This will open up the space of Retzius
3. Identify Hesselbach’s triangle and the three potential sites of herniation related to it (direct, femoral, obturator)
4. Identify and elevate the epigastric vessels
5. Bluntly develop the space of Bogros to the level of the ASIS
6. Dissection of cord structures
7. Placement of mesh
Step 1
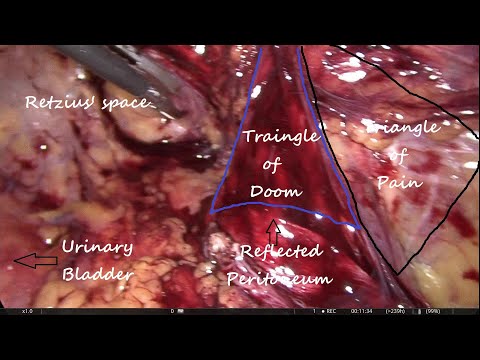
The first step is to identify the pubic symphysis in the midline. The pubic symphysis serves as an important landmark to orient the surgeon especially in complex cases. The bladder is posterior to the pubic symphysis and care must be made not to injure it when dissecting posterior to the pubic symphysis.
Step 2
Cooper’s ligament is bluntly swept clear in a medial to lateral direction while staying close to the ligament and close to the bone in a gentle and controlled manner. This will allow visualization of the femoral and obturator spaces. If a femoral or obturator hernia is encountered, they are reduced bluntly. Care must be made during reduction of femoral hernias to avoid injuring the femoral vein or the occasional corona mortis artery. Full dissection of the space of Retzius is achieved by dissecting the contralateral Cooper ligament thereby ruling out a femoral, direct and obturator hernia as well on the contralateral side.
Step 3
The direct space (Hesselbach’s triangle) is identified immediately superior to the femoral space and separated by the medial aspect of the iliopubic tract. A direct hernia normally obscures the view to Cooper’s ligament and is readily identifiable during the initial dissection. A convexity or a bulge in Hesselbach’s triangle signifies the presence of a large indirect hernia. A direct hernia sac is reduced by peeling it away from the attenuated transversalis fascia and using constant and gentle traction and counter-traction
Figure 6 Reduction of direct, indirect sacs and cord lipomas. (A) Reduction of direct sac; (B) reduction of cord lipoma; and (C) reduction of indirect sac.
Step 4
The epigastric vessels are identified and elevated anteriorly.
Step 5
While elevating the epigastric vessels, the space of Bogros is developed using horizontal blunt dissection. The space is developed laterally to the level of the anterior superior iliac spine (ASIS) to allow placement of an appropriately sized mesh.
Step 6
The indirect space is now identifiable by finding the cord structures in men or round ligament in women passing through the internal ring and lateral to the epigastric vessels. The indirect sac can be seen overlying the cord structures or round ligament. If it is not possible to identify the vas deferens or the round ligament immediately next to the epigastric vessels, then an indirect hernia is present. Prior to reduction of the indirect sac, it is important to look for and reduce cord lipomas that are found in the upper and outermost quadrant of the internal rings. Their reduction allows more working space and better identification of the edge of the indirect sac (Figure 6B). Reduction of the sac is accomplished by sweeping the cord structures or round ligament posteromedially while holding the sac superolaterally.
Step 7
Numerous mesh products for inguinal hernia repair are available. Our preference is a 15 cm2 sheet of medium weight polypropylene that is trimmed to an appropriate shape and size, rolled and introduced into the space of Retzius through the Hasson port. The mesh is then unrolled and should extend from the midline to the ASIS and cover all hernia spaces (Figure 7). The mesh should be placed in the visceral plane of the extraperitoneal fascia in the space of Bogros to avoid contact with the nerves. No slit is placed in the mesh as this has been shown to be a factor in recurrences. We do not routinely tack the mesh in place. However, some may find it helpful to place a single tack in Cooper’s ligament to facilitate unrolling of the mesh. Also, and to ensure adequate medial overlap, tacking may be needed in the case of large direct and femoral hernias.
#surgery #doctor #medicine #medical #surgeon #health #doctors #nurse #healthcare #medicalstudent #anatomy #surgical #covid #medico #shivkumarbunkar #jlnhospitalajmer |
| Category |
People & Blogs |
| Tags |
People & Blogs Download MP4 | People & Blogs Download MP3 | People & Blogs Download MP4 360p | People & Blogs Download MP4 480p | People & Blogs Download MP4 720p | People & Blogs Download MP4 1080p |
More Videos