EXTRACRANIAL to INTRACRANIAL HIGH FLOW BYPASS FOR WORLD ‘S LARGEST CAVERNOUS ICA ANEURYSM
Hellow guys, Welcome to my website, and you are watching EXTRACRANIAL to INTRACRANIAL HIGH FLOW BYPASS FOR WORLD ‘S LARGEST CAVERNOUS ICA ANEURYSM. and this vIdeo is uploaded by Dr Shivashankar Marajakke at 2024-01-13T07:31:39-08:00. We are pramote this video only for entertainment and educational perpose only. So, I hop you like our website.
Info About This Video
| Name |
EXTRACRANIAL to INTRACRANIAL HIGH FLOW BYPASS FOR WORLD ‘S LARGEST CAVERNOUS ICA ANEURYSM |
| Video Uploader |
Video From Dr Shivashankar Marajakke |
| Upload Date |
This Video Uploaded At 13-01-2024 15:31:39 |
| Video Discription |
#Brain Bypass(EC-IC) - for World’s Largest Cavernous ICA ( Internal carotid artery ) #Aneurysm.
Bypass in brain is very challenging & demands highest levels of skills in view of very small vessels , narrow space with eloquent brain parenchyma around and carry life threatening consequences if erred . Hence very rarely done by very few surgeons (less than 1% of neurosurgeons ) across the world .
HISTORY
49 year old female with no known co morbid illnesses presented with H/O sudden onset drooping of left eyelid with loss of vision 8 years back and now with H/O sudden vision worsening in right eye , profuse nasal and jaw bleed of 8 days .
On further enquiry , husband revealed that 8 years back she was evaluated in one of the central neuro institute and was advised surgery after some angiogram and baloon test ( no details available) . But for some technical reasons at that time , surgery could not be done .
ON EXAMINATION
GCS 15/15 , left eye ptosis and mild proptosis .
Bilateral eye - no perception of light .
Left maximally pulsatile swelling .
Left maximally region ( under the cheek ) pulsatile bulge/swelling .
INVESTIGATIONS
CT ANGIO - Showed a very large aneurysm noted arising from the horizontal segment of cavernous segment of left internal carotid artery measures about 10.5 cm in cranio-caudal extent x 7.5cm in antero- posterior
x 5.9cm in transverse dimension. The patent lumen of the aneurysm shows avidly enhancing area measures about 4.3 x 2.9 x 2.8cm- thrombus .
Treatment STRATEGY
1)DSA ,baloon occlusion test and plan for flow diverter/ trapping .
In view of financial issues - they deferred the above option.
2)Surgery - A) Extra-cranial - intracranial Bypass using Radial artery graft .
B)Trapping of aneurysmal segment of ICA
STEPS Of EC-IC BYPASS .
After general anesthesia. Patients head is placed in a 3-pin, Mayfield skull-fixation device, which attaches to the table. Painting and draping of scalp , left side neck and upper limb is done. .
1)Harvesting Radial artery graft ( RAG) from left hand ( after normal arterial Doppler study ) . Branches arising form vessel are clipped preparing it for anastomosis . Graft filled with heparinised saline to prevent thrombosis .
2)Exposure of neck to expose ICA ( internal carotid artery ) for ligation and ECA ( external carotid artery ) for anastomosis. They are exposed in the neck through an incision below mandible .
3)Question mark skin incision made to expose left fronto-temporal region . Superficial temporal artery exposed and temporalis muscle raised. .
4)Craniotomy and Clinoidal drilling done to expose the proximal ICA ( ophthalmic segment ) for trapping aneurysm . After burrhole , craniotomy is done . The bone flap is lifted and removed to expose the the dura. The dura is opened and folded back to expose the brain.
5)Dissection of arachnoid to expose ICA and M2 inferior trunk for anastomosis . Working under an operating high end microscope, the surgeon carefully locates a branch of the middle cerebral artery (MCA) suitable for bypass. The size of the recipient vessel must be a good match for the diameter of the donor vessel.
6)Tunnelling of radial artery graft(RAG) from neck to brain using chest tube - check to avoid kinking
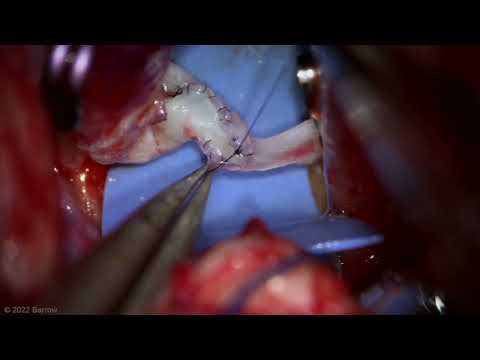
7)Anastomosis of inferior trunk of M2 to RAG (Radial artery graft )and confirming the patency. Temporary clips are placed across the donor and recipient vessels to stop the blood flow. The graft vessel is cut and the end prepared for anastomosis. The surgeon then makes an opening in the side of the MCA vessel and sutures the two blood vessels together.
8)Anastomosis of ECA with RAG after temporary clip over graft proximally
9)Ligation of ICA in the neck
10)permanent Clipping of ophthalmic segment ICA
11)Confirmation of graft patency using Doppler . After the vessels are anastomosed , the surgeon releases the temporary clips and verifies there are no leaks.
12)Aspiration of blood from trapped segment of ICA - this collapses the size of fundus of aneurysm. .
13)Closure of wounds .
POSTOPERATIVE PERIOD
Patient extubated on table , neurologically no fresh deficits .
Postop CT Angiogram study
Complete non filling of aneurysmal segment of ICA and satisfactory graft patency with very good flow .
Patient discharged in good condition on postop Day 10 after suture removal. She is neurologically and vitally stable .Right eye vision is gradually improving .
CONCLUSION
With Proper understanding of disease , strategic planning , finest technological ( infrastructure) support , skilled Neurosurgeon/ Neuro anaesthetist and OT /ICU team , any kind of complex challenging procedures and best of results can be achieved .
With such a state of art Neuro set up , we are one among very few centres of India for rare, complex and challenging epilepsy surgeries , endoscopic brain surgeries and such complex neuro vascular surgeries- offering them beyond financial barriers . |
| Category |
People & Blogs |
| Tags |
People & Blogs Download MP4 | People & Blogs Download MP3 | People & Blogs Download MP4 360p | People & Blogs Download MP4 480p | People & Blogs Download MP4 720p | People & Blogs Download MP4 1080p |
More Videos